Dry Socket After Wisdom Teeth Removal: Symptoms, Prevention, and Treatment
Dry socket is the most painful complication after wisdom teeth removal — and one of the most preventable. Learn the symptoms, causes, treatment options, and how PRF helps prevent it.
Dry socket wisdom teeth
Dry socket is the complication wisdom teeth patients dread most — and for good reason. It is genuinely painful. It can extend recovery by several days. And despite how common it is in general extraction statistics (affecting 2–5% of all extractions), it is largely preventable with the right post-operative protocol and, when it does occur, it is completely treatable.
This guide covers everything patients need to know about dry socket: what it actually is, what causes it, how to recognize it early, what the treatment involves, and the measures — including PRF — that significantly reduce the risk of it happening in the first place.
What Is Dry Socket? The Direct Definition
Dry socket (alveolar osteitis) is a post-extraction complication that occurs when the blood clot that normally forms in the tooth socket is dislodged, dissolves prematurely, or fails to form — leaving the underlying bone and nerve endings directly exposed to air, food, and bacteria.
The name is literal: the socket looks dry when examined, with visible bone where the dark clot should be. This exposed bone is the source of the distinctive pain.
What Causes Dry Socket?
Dry socket results from disruption of the blood clot. The most common causes:
Suction
This is the leading mechanical cause. Using a straw, smoking a cigarette, vaping, or even vigorous rinsing or spitting creates negative pressure in the oral cavity that can literally pull the clot out of the socket. This is why the 'no straws' instruction is the single most-emphasized post-operative rule after wisdom teeth removal.
Smoking and Tobacco Use
Smoking increases dry socket risk through two distinct mechanisms: the suction involved in drawing on a cigarette or vape, and the chemical and thermal effects of tobacco smoke on the healing socket environment. Nicotine constricts blood vessels, reducing blood flow to healing tissue. Studies consistently show that smokers have 3–5 times higher dry socket incidence than non-smokers following extractions.
Oral Contraceptives
Estrogen-containing oral contraceptives affect clotting factor levels and have been associated with higher dry socket incidence. This is a legitimate clinical risk factor that patients on hormonal birth control should discuss with their surgeon during pre-operative consultation. Some surgeons recommend scheduling extraction during the low-estrogen phase of the cycle.
Complex or Traumatic Extraction
More complex surgical extractions — particularly impacted lower wisdom teeth requiring bone removal and tooth sectioning — involve greater surgical trauma and create larger sockets. Both factors increase dry socket risk compared to simple erupted tooth extraction.
Poor Post-Operative Compliance
Eating hard or crunchy foods too soon, vigorous rinsing within the first 24 hours, brushing directly over the extraction site, or failing to take prescribed antibiotics when indicated all increase the risk that the clot will be disturbed or that bacterial contamination will undermine socket healing.
IN-ARTICLE IMAGE PROMPT — NORMAL HEALING VS. DRY SOCKET VISUAL
Clean split-panel educational illustration (dark navy background, premium dental brand aesthetic). Two side-by-side panels, each showing a simple cross-section of a tooth socket (post-extraction view from the front). LEFT panel labeled 'Normal Healing — Days 3-5': socket contains a dark reddish-maroon fill (representing stable blood clot), surrounded by healthy pale-pink gum tissue. A small checkmark icon in the top corner (light teal). RIGHT panel labeled 'Dry Socket (Alveolar Osteitis)': socket is empty/open, showing white-grey bone texture at the bottom. The surrounding gum tissue has a slightly inflamed appearance (warmer pink). A small warning icon in the top corner (amber/orange). Both panels have matching clean borders, same scale, same socket shape. Simple line art with minimal color fills. Clinical but accessible. Wide 16:9 format.
How Common Is Dry Socket?
Dry socket affects approximately 2–5% of all tooth extractions and up to 10–12% of lower wisdom teeth extractions specifically (where it is most common due to anatomy and blood supply characteristics). In smokers, that figure rises to 25–30% in some study populations.
By comparison, upper wisdom teeth extraction carries a much lower dry socket risk — typically under 2% — due to differences in blood supply and socket anatomy.
At Dr. Wisdom Teeth, the inclusion of PRF in every procedure is specifically designed to address this risk profile — particularly for lower wisdom teeth extractions.
Dry Socket Symptoms: How to Know If You Have It
The hallmark of dry socket is pain that worsens rather than improves, typically appearing 3–5 days after surgery. This timing is clinically important: day 1–2 post-extraction pain is expected and normal. Pain that escalates after this initial window — especially if it becomes throbbing or radiating — is a warning sign.
The Defining Symptom Pattern
Onset timing: Days 3–5 after extraction (occasionally as early as day 2 or as late as day 7).
Pain character: Throbbing, aching, or radiating pain at the extraction site. Often described as significantly worse than expected and different in quality from normal post-surgical soreness.
Radiation pattern: Pain frequently radiates to the ear, temple, eye, or neck on the affected side — following the distribution of the inferior alveolar nerve for lower extraction sites.
Visual sign: If you look at the socket (with a flashlight and mirror), you may see a whitish-grey appearance or visible bone where the dark clot should be.
Bad taste or odor: Bacterial activity in the exposed socket frequently produces a foul taste or unpleasant odor not explained by food debris.
Dry Socket vs. Normal Post-Extraction Pain: How to Tell the Difference
This distinction matters — normal recovery discomfort should not prompt an emergency call, but dry socket should not be waited out.
Normal healing pain: Gradually improves after day 1–2. Managed adequately with prescribed or OTC pain medication. Does not radiate significantly. No worsening trend.
Dry socket pain: Worsens or plateaus after the first 3 days. Radiates to the ear, jaw, or temple. Not adequately controlled by over-the-counter medication alone. Associated with a bad taste or odor. Possibly visible bone in the socket.
If you suspect dry socket, contact your surgeon promptly. Dry socket does not resolve on its own without treatment — and the sooner it is treated, the sooner you get relief.
Think you might have dry socket? Don't wait it out. Call (801) 370-0050 — Mon–Fri 8am–5pm. Same-day evaluation available at both Provo and Murray locations.
Dry Socket Treatment: What Actually Happens
Dry socket is treatable. Treatment provides rapid, meaningful pain relief — usually within hours. Here is what the clinical process looks like:
Step 1: Irrigation and Cleaning
The exposed socket is gently irrigated to remove any debris, bacteria, or decomposed clot material. This is not painful — the socket is already exposed, and gentle saline irrigation is soothing rather than aggravating.
Step 2: Medicated Dressing Placement
A medicated dressing — typically containing eugenol (clove oil) or a similar analgesic agent — is placed directly into the socket. Eugenol has established anesthetic properties in dental tissue and provides direct, localized pain relief at the exposed bone surface.
Most patients report meaningful pain relief within 30–60 minutes of dressing placement. The relief is often described as dramatic compared to the preceding pain.
Step 3: Dressing Changes
The dressing typically needs to be replaced every 2–5 days until the socket begins forming healthy granulation tissue on its own. Most dry socket cases require 2–4 office visits over 1–2 weeks. Each visit involves removing the old dressing, re-irrigating, and placing a fresh medicated dressing.
Additional Support
Your surgeon may also prescribe or recommend:
Prescription-strength pain medication to bridge between dressing visits
Antibiotics if there is evidence of secondary infection alongside the dry socket
A take-home irrigation kit to gently flush the socket between visits
How to Prevent Dry Socket: The Complete Protocol
The prevention protocol for dry socket is one of the clearest post-operative instructions in dentistry. These are not suggestions — each item has a direct clinical rationale.
The Non-Negotiables (Days 1–7)
How PRF Reduces Dry Socket Risk
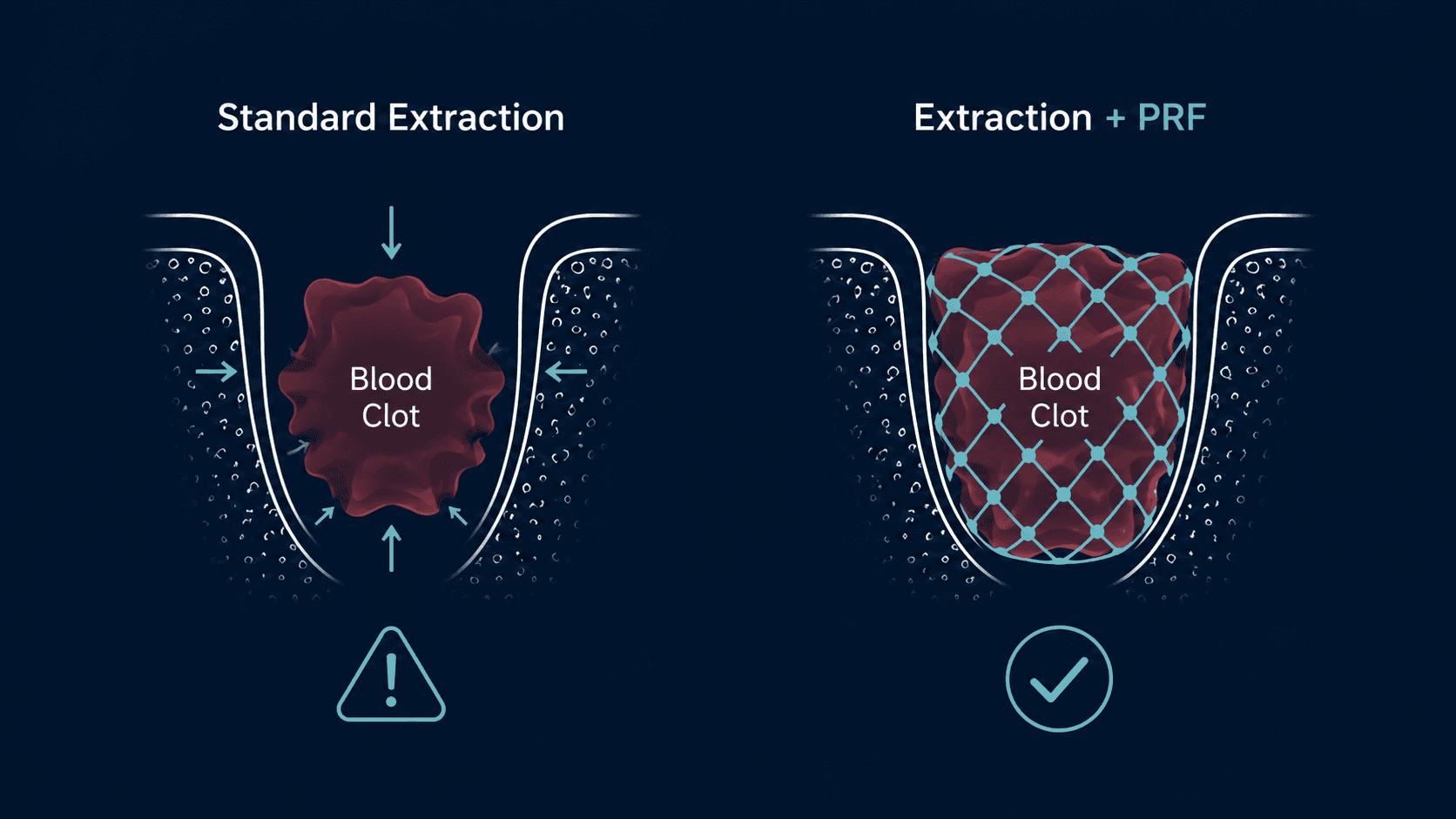
Among the clinical tools available to reduce dry socket incidence, PRF (Platelet-Rich Fibrin) has the strongest evidence base and the most direct mechanism of action.
PRF is a fibrin matrix made from the patient's own blood, placed in the extraction socket during surgery. The fibrin network physically reinforces the blood clot — making it more stable and more resistant to the forces (mechanical, chemical, and bacterial) that lead to clot loss.
Multiple randomized controlled trials have demonstrated statistically significant reductions in dry socket incidence in lower wisdom teeth extractions when PRF is used versus standard extraction without PRF. The effect is most pronounced in high-risk patients — smokers, patients with impacted lower wisdom teeth, and patients with a history of dry socket.
At Dr. Wisdom Teeth, PRF is included in every procedure. It is not an elective add-on or a premium tier. The practice was built around wisdom teeth surgery specifically, and PRF is a clinical standard of care in that specialty context.
Frequently Asked Questions
How long does dry socket pain last?
Untreated dry socket pain can persist for 7–10 days or longer as the socket slowly granulates on its own — a painful and unnecessary process. With treatment (medicated dressing placement), significant pain relief typically occurs within hours of the first office visit. Most patients complete treatment within 1–2 weeks of dressing changes.
Can dry socket heal on its own without treatment?
Yes — eventually. The socket will granulate and heal even without treatment. But the process is significantly more painful and takes considerably longer than with clinical management. There is no good reason to tough out dry socket when treatment is straightforward and provides rapid relief.
I used a straw once on day 2. Do I definitely have dry socket?
Not necessarily. A single straw use does not guarantee dry socket — but it does increase the risk. Monitor the extraction site. If pain begins to worsen rather than improve over the next 24–48 hours, have the site evaluated.
Can I get dry socket in upper wisdom tooth sockets?
Yes, but it is significantly less common than in lower sockets. Upper wisdom tooth sockets have better blood supply and different anatomy, making them more resistant to clot loss. Lower sockets — particularly impacted lower wisdom teeth requiring surgical extraction — carry the highest risk.
Is dry socket an infection?
Dry socket is technically not an infection — it is an inflammatory condition resulting from clot loss. However, bacterial contamination of the exposed socket can occur concurrently or as a secondary development, and antibiotics may be prescribed alongside the dressing treatment when infection is present. If you have fever or rapidly increasing swelling alongside dry socket symptoms, those signs point toward infection and warrant prompt evaluation.
Will I definitely get dry socket if I smoke?
Not definitely — but your risk is substantially elevated. Studies show 25–30% dry socket incidence in smokers following lower wisdom teeth extraction, compared to 2–5% in non-smokers. The combination of smoking with PRF inclusion significantly reduces this risk compared to smoking with standard extraction alone — but abstaining from smoking for at least 72 hours post-surgery remains the single most impactful thing a smoker can do to protect their recovery.
I had dry socket before. Will I get it again?
Prior dry socket is a risk factor for recurrence. Let your surgical team know about this history before your procedure. PRF inclusion, careful attention to post-operative instructions, and — if you smoke — tobacco abstinence are all particularly important for patients with a prior dry socket history.
The Bottom Line
Dry socket is real, painful, and common enough that every wisdom teeth patient should understand it before surgery — not after. The good news is that the prevention protocol is clear and the risk is manageable. Follow the post-operative instructions precisely. No straws. No smoking. Soft foods. Stay hydrated.
When prevention is supported by PRF placement — which reinforces the clot structurally from the moment surgery ends — dry socket risk drops meaningfully. At Dr. Wisdom Teeth, this is built into every procedure, at both Provo and Murray locations.
If you develop symptoms that suggest dry socket at any point in your recovery, contact the office. Treatment is straightforward, quick, and provides real relief.
Schedule your procedure or get a post-op concern evaluated: drwisdomteeth.com | (801) 370-0050 | Mon–Fri 8am–5pmProvo: 2230 N University Pkwy #8A | Murray: 5888 S 900 E #101

Written by
Dr. Wisdom Teeth
Resources


