
Best Age to Get Wisdom Teeth Removed: What Oral Surgeons Actually Recommend
Is there a best age for wisdom teeth removal? Yes — and it matters more than most people realize. Learn what changes at each age bracket and why early usually means easier.
Teen Concerns, Adult Concerns, Common Questions, Timing, Surgery
The question of when to get wisdom teeth removed doesn't have one universal answer — but it does have a clear framework backed by decades of clinical experience. Age matters in wisdom teeth surgery. It affects how complex the procedure is, how fast you heal, and how much risk is involved. This guide breaks down what actually changes at each age bracket, what the clinical consensus recommends, and why 'I'll deal with it later' tends to mean 'I'll deal with a harder version of this later.'
The Short Answer: What Oral Surgeons Recommend
The optimal window for wisdom teeth removal is generally between ages 17 and 25. Root development is not yet complete, bone is less dense, recovery is faster, and complications are least common. This is the stage where the procedure is most straightforward and outcomes are most consistently smooth.
That said, wisdom teeth removal is performed safely and routinely in patients in their 30s, 40s, and beyond — the procedure is more complex, but it is not out of reach. The goal of this guide is to help patients at every age understand their situation accurately.
Why Age Matters in Wisdom Teeth Surgery: The Underlying Biology
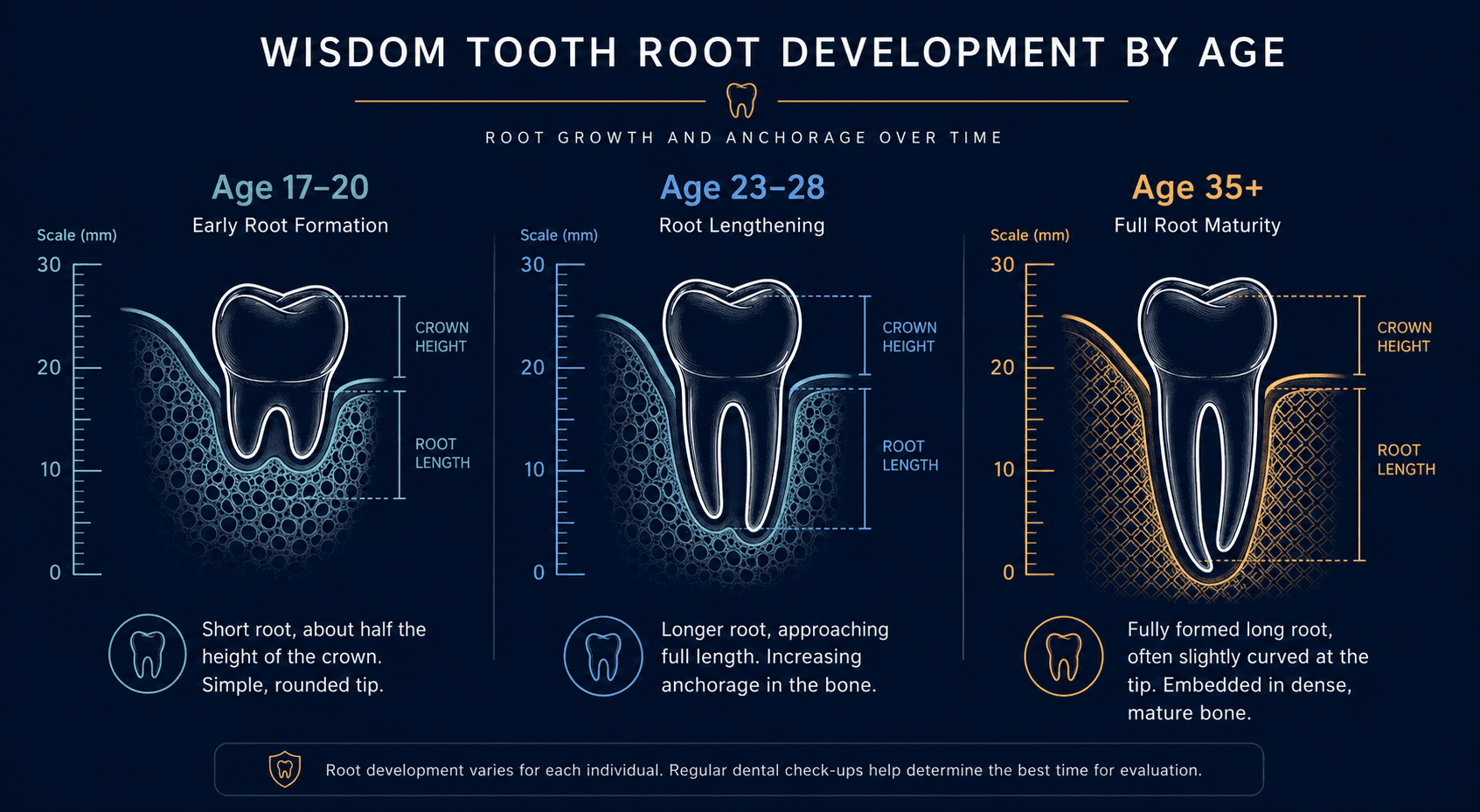
Root Development
Wisdom tooth roots continue to grow and lengthen through the early-to-mid twenties. At 17–19, the roots are typically one-half to two-thirds of their final length. At 24–28, they may be fully formed. At 35+, they are fully anchored in dense, mature bone.
Shorter, less-developed roots are simpler to remove. They require less bone removal, less force, and create smaller sockets. Longer, fully-formed roots in dense bone require more technique to extract — particularly if they are curved, divergent, or close to the inferior alveolar nerve in the lower jaw.
Bone Density
Bone density in the jaw increases with age, as it does throughout the body. Younger bone has a more flexible, compliant quality that makes tooth removal more predictable. Older bone is harder, more brittle in some respects, and requires more controlled surgical force. This is why post-operative swelling and trismus (jaw stiffness) tend to be more pronounced in older patients — the surgical procedure is simply more demanding on the surrounding tissue.
Healing Rate
Cell turnover, tissue regeneration, and blood supply to healing sites are all more vigorous in younger patients. The same socket that takes 7–10 days to functionally heal at age 19 may take 10–14 days at age 35 and potentially longer at 45+. This is not a complication — it is normal physiology — but it has practical implications for recovery time planning.
Risk of Complications
The two most clinically significant complications of lower wisdom teeth removal — dry socket and nerve-related numbness — both have higher incidence in older patients. The inferior alveolar nerve, which runs through the lower jaw and provides sensation to the lower teeth, lip, and chin, is more likely to be closely associated with fully-developed lower wisdom tooth roots than with shorter, developing roots in teenagers.
Age-by-Age Breakdown: What to Expect
Ages 16–18: Early Evaluation, Not Always Immediate Removal
At 16–18, wisdom teeth may not yet be fully visible on X-ray or may just be beginning to emerge. The right approach at this age is evaluation — a panoramic X-ray to assess the position and trajectory of all four third molars.
Not every 16-year-old needs immediate removal. What the evaluation determines:
Whether the wisdom teeth are developing normally or showing early signs of impaction
Whether there is adequate space in the jaw for eruption (rarely the case in modern populations)
Whether removal is advisable now — proactively — or whether monitoring is appropriate for another 1–2 years
For many patients, age 17–18 is the ideal time to remove wisdom teeth that are clearly going to cause problems — before roots develop further and while recovery is fastest. High school summer break is a popular and practical window.
Ages 19–25: The Clinical Sweet Spot
Most oral surgeons consider 18–24 the optimal window for wisdom teeth removal when it is indicated. Root development is in a favorable stage — substantive enough that the teeth are accessible, incomplete enough that they aren't fully anchored. Bone is healthy and responsive. Recovery moves quickly. Anesthesia management in this age group is predictable and low-risk.
The vast majority of wisdom teeth procedures performed at Dr. Wisdom Teeth fall in this age range, and outcomes are consistently smooth when post-operative instructions are followed.
Ages 26–35: Still Routine, Slightly More to Plan
Patients in their late twenties and early-to-mid thirties are well within the range for routine wisdom teeth removal. The procedure is more complex than at 19, recovery may take a few days longer, and post-operative swelling tends to be more pronounced — but these are relative differences, not absolute barriers.
Patients in this bracket often have impacted wisdom teeth that have been monitored for years. If monitoring has revealed no pathology and the teeth remain asymptomatic, some may continue monitoring with close follow-up. If there is any evidence of adjacent tooth impact, periodontal involvement, cyst formation, or recurring pericoronitis, removal is the appropriate recommendation.
Ages 35–45: Individual Assessment Required
Root development is complete. Bone is denser. The inferior alveolar nerve is more likely to be in close proximity to fully-formed lower roots. For fully bony impacted teeth with no associated pathology and no symptoms, some clinicians recommend continued monitoring rather than prophylactic removal.
However, the assumption that 'asymptomatic means fine' deserves scrutiny. Research shows that wisdom teeth in this age group continue to accumulate risk for adjacent tooth root resorption, periodontal disease, and cyst development — silently. A current panoramic X-ray is the only honest way to assess this.
For partially erupted or symptomatic wisdom teeth at this age, removal is almost always the appropriate intervention. The surgery is more complex but is performed routinely and safely by experienced oral surgery teams.
Age 45+: Surgical Judgment, Not Automatic Monitoring
At 45 and beyond, each case must be assessed on its own clinical merits. Fully bony impacted teeth with no evidence of pathology on current imaging in an otherwise healthy patient may genuinely be appropriate to leave in place. But this conclusion should be reached through active clinical reasoning — not through inertia or assumption.
Partially erupted symptomatic teeth, teeth with associated cysts or root resorption of adjacent teeth, or teeth causing recurrent infection should be addressed regardless of age. The risk of surgery must be weighed against the ongoing and accumulating risk of non-treatment.
Not sure whether your wisdom teeth need to come out now? We evaluate each case individually. Call (801) 370-0050 or book a consultation at drwisdomteeth.com.
The Risk of Waiting: What Accumulates Over Time
Root Resorption of Adjacent Teeth
A wisdom tooth pressing against the root of the adjacent second molar can cause external root resorption — the dissolution of the neighboring tooth's root structure. This process is slow but irreversible. The second molar may become unsalvageable in advanced cases. This is a preventable outcome that becomes an expensive and painful outcome when action is delayed too long.
Dentigerous Cysts
Fluid-filled cysts can develop around impacted, unerupted wisdom teeth over time. They are rarely present at age 18 and increasingly common with delayed removal. Small cysts are treated with simple excision alongside the extraction. Large cysts require more extensive procedures — sometimes including bone grafting and longer recovery.
Increasing Surgical Complexity
This is the most direct cost of waiting. Every year that passes with wisdom teeth in place adds marginally to the complexity of the eventual procedure. The aggregate effect of several years of delay — particularly through the late twenties and thirties — is meaningful. A procedure that would have taken 45 minutes at 20 may take 75–90 minutes at 40, with greater post-operative swelling, longer recovery, and higher risk of nerve proximity complications.
Common Reasons People Delay (And the Reality of Each)
'They don't hurt.' Pain is a lagging indicator, not a leading one. Significant structural damage can occur without pain.
'My dentist said to monitor.' Monitoring is sometimes the right call — and sometimes a comfortable default. Ask specifically: what are we monitoring for, at what interval, and what would trigger a removal recommendation?
'I'm worried about recovery time.' Recovery time is shorter at a younger age, not longer. Waiting extends future recovery, not the current one.
'It's expensive.' Removal now, at lower complexity, is almost always less expensive than removal later at higher complexity — especially if adjacent tooth damage or cyst management is involved.
A Note on Early Evaluation for Teenagers
The recommendation to have wisdom teeth evaluated starting around age 16–17 is not about rushing into surgery. It is about having accurate information early — knowing what's happening with the teeth, what trajectory they're on, and what the optimal timing for intervention is. A panoramic X-ray and a brief consultation with an oral surgeon is a 30-minute investment that answers years of 'should I be doing something about this?'
At Dr. Wisdom Teeth, parents frequently bring teenagers in for this initial evaluation. The team reviews current imaging, explains what is visible, and gives a clear recommendation — including whether to wait, monitor, or proceed. There is no pressure to commit to surgery at the evaluation appointment.
Frequently Asked Questions
My teenager is 16 — is it too early to remove wisdom teeth?
It depends on what the X-ray shows. If the wisdom teeth are clearly impacted and root development is already underway, age 17–18 may be the ideal time to act. If roots are very early in development, waiting 1–2 years and reassessing makes sense. An evaluation answers this question specifically.
I'm 38 and my wisdom teeth have never caused problems. Should I still have them removed?
Not necessarily — but 'they've never caused problems' doesn't mean they aren't causing subtle damage. Get a current panoramic X-ray. If there is no evidence of cyst, adjacent tooth root resorption, bone loss, or periodontal involvement around the third molar sites, a decision to continue monitoring is reasonable. If any of those findings are present, removal is worth seriously considering regardless of age.
Is wisdom teeth removal more dangerous at older ages?
'More complex' is more accurate than 'more dangerous.' The risks of the procedure — anesthesia, bleeding, nerve proximity — are manageable at any age in a healthy patient. The complexity of the extraction itself increases with age due to root development and bone density. An experienced oral surgery team factors this into the surgical approach for each individual case.
Can wisdom teeth grow in normally without problems?
Yes — occasionally. Patients with larger jaws and wisdom teeth in favorable positions can sometimes fully erupt without impaction or crowding. But this is the exception. Approximately 85% of people will eventually need their wisdom teeth removed, according to studies on third molar eruption patterns in modern populations.
Is it okay to remove all four wisdom teeth at once?
Yes — and it is the standard approach at Dr. Wisdom Teeth. Removing all four at once means a single anesthesia event, a single recovery period, and a single period away from work or school. Spreading the procedure across multiple sessions means multiple recoveries. Unless there is a specific clinical reason to stage the procedure, one appointment for all four is strongly preferred by most patients and clinical teams alike.
The Bottom Line
There is a best time for wisdom teeth removal, and that window is real — not a sales construct. Root development, bone density, healing rate, and complication risk all move in one direction over time, and waiting does not improve the situation. The patients who regret acting on wisdom teeth removal are rare; the patients who regret waiting are not.
If you're in the optimal window and haven't evaluated yet, now is the time. If you're past it and still have your wisdom teeth, the answer is an honest assessment of your current situation — not a default to waiting.

Written by
Dr. Wisdom Teeth
Resources


